 In this section
In this section

Meet the Manchester Bladder Exstrophy Team
Consultant Paediatric Urologists (Prof Max Cervellione, Mr David Keene and Ms Arianna Mariotto)


Senior Urology Nurse Specialist (Jen Powell)

Consultant Orthopaedic Surgeon (Mr Farhan Ali and Mr Emmanouil Morakis)

Clinical Psychologists (Ruth Hurrell, Lucy Ferguson)


Consultant Adult Urologist (Mr Ian Pearce)

Consultant Adolescent Gynaecologist (Miss Gail Busby and Ms Sujata Gupta)


Play Specialist (Yvie Morley)

Consultant Paediatric Anaesthetists (Dr Jai Sivaprakasam, Dr Anju Bendon)
What is Bladder Exstrophy, Epispadias and Cloacal Exstrophy?
These conditions are part of a spectrum of birth defects, with Epispadias being at the minor end of the spectrum, and Cloacal Exstrophy being the most severe form. Approximately 40% of Bladder and Cloacal Exstrophy defects are detected on ante-natal scan, but the condition can often be missed due to timings of scans and positioning of the foetus, making it harder to identify on a routine ante-natal scan.
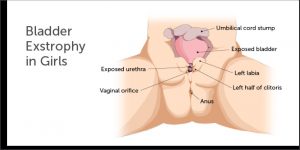
Classic Bladder Exstrophy is an abnormality of the lower part of the tummy where the bladder, urethra (the tube that takes urine to the outside of the body), the pelvic bone and the genitals are affected. The bladder is seen on the outside of the baby’s tummy. The urethra is open along the top and is not formed into a cylindrical tube as it should be, and the tummy button is in a lower position. The pelvic bones do not come together completely at the front (this is known as pubic diastasis). In boys, the penis is tilted backwards and is often shorter and wider than normal. In girls the clitoris is split.
Diagram showing male bladder exstrophy & epispadias
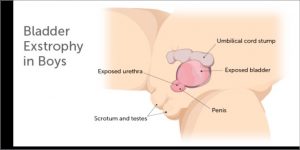
Diagram showing female bladder exstrophy & epispadias
Epispadias is a less extensive form of the condition. The bladder is not visible outside the tummy but the urethra (the tube that takes urine to the outside of the body), is open on the top side and is not formed into the cylindrical tube shape as it should be. In girls, the clitoris and labia is split. Epispadias is always present in both Bladder Exstrophy and Cloacal Exstrophy, however it is possible to see Epispadias on its own (without Bladder Exstrophy or Cloacal Exstrophy).
Diagram showing male primary epispadias
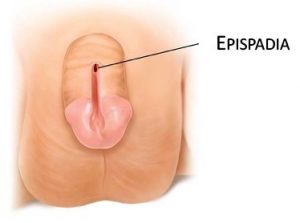
Diagram showing female primary epispadias

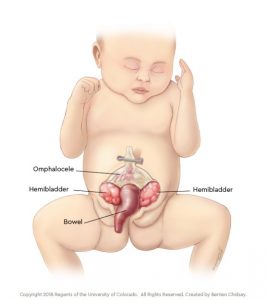
In Cloacal Exstrophy, the bowel and bladder are both seen on the outside of the baby’s tummy.
What happens first?
Bladder Exstrophy & Epispadias are corrected in a series of operations over the first years of life. The overall aim of treatment is to protect the kidneys and correct the abnormalities, so that your child’s urinary system and genitals work properly and look as normal as possible.
If your baby has been born with Cloacal Exstrophy, an operation to ensure that your baby can pass faeces will usually be performed in the first week of life. You will meet with the Consultant Paediatric Urologist and our specialist team who will explain the operation. The anatomical abnormalities to the urethra, genitals and bladder will not be corrected within the same operation but will thereafter follow a similar structure and timing of surgeries as those born with Bladder Exstrophy & Epispadias.
If your baby has been born with Bladder Exstrophy & Epispadias, the operation to close the tummy is often done around 4-6 months after birth. This gives your baby the time to grow and mature, making surgery much safer. You will be shown how to take care of your baby’s tummy after birth, and can usually be discharged home after a few days, providing baby is otherwise fit and well. We believe that having the opportunity to get to know your new baby and spend time together in your own environment is of benefit for the whole family. Our clinical evidence shows that closing the tummy when baby is a little bit older has no impact on their overall outcome and continence
Your baby will need to have some blood tests, a medical photograph and an ultrasound scan of the kidneys before they are discharged home. This checks that your baby’s kidneys are working well, and documents how their tummy looked when they were born. Your baby will also need to have some special scans of the pelvis (CT/MR) but this is often done once a date for closing the tummy has been scheduled. Your baby may need to be given medicines to keep them still whilst the scans are completed.
Once our team at Royal Manchester Children’s Hospital have been informed of the birth of your baby and their diagnosis, we will arrange an out-patient appointment for you to attend our clinic to meet the team and will be provided telephone support by our clinical nurse specialist. If your baby was diagnosed ante-natally (on a scan), then you may be offered to meet us in clinic before baby is born. When we all agree baby is ready for the surgery, we will list them and a date for them to come in will be allocated by the theatre scheduler.
Each patient’s condition is unique and the information above is a guide and will be individualised for each patient.
Resources
We have created a series of patient information leaflets which can be downloaded by clicking on the links in the right-hand menu.